
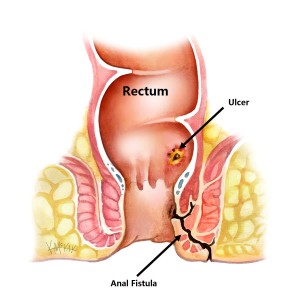
Our surgeons specialise in the assessment and surgical management of all types of anal fistulae. Treatment is tailored to each individual, with the goal of clearing infection, promoting healing, and preserving normal bowel control.
Initial Management of an Anal Fistula
The first step in managing an anal fistula is careful assessment and control of infection (sepsis).
Assessment
Initial assessment aims to identify the internal opening of the fistula and determine how much of the anal sphincter muscle is involved. This may be done:
⦁ At the bedside using a digital rectal examination and proctoscopy, or
⦁ Under general anaesthetic for a more detailed examination
In some cases, an MRI scan is required. MRI has been shown to be highly accurate in defining fistula anatomy and guiding treatment decisions [1].
Drainage and Infection Control
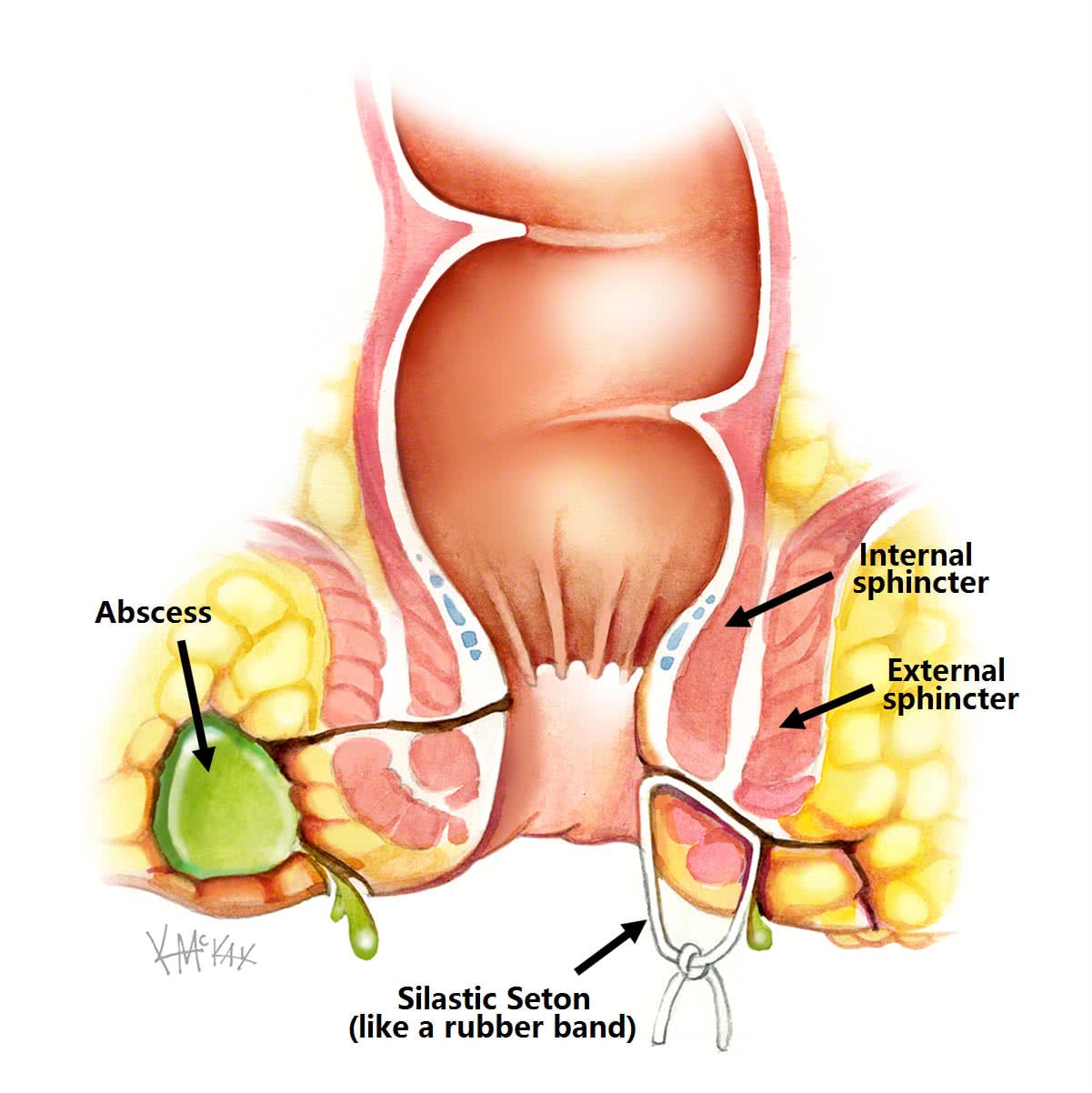
If there is ongoing infection or an associated abscess, drainage is essential. This is commonly achieved by inserting a silastic seton drain.
A seton is a thin, flexible loop (similar in size and consistency to a rubber band) that is placed through the fistula tract during a short operation under general anaesthetic. It is tied in place to allow continuous drainage of pus and fluid, helping inflammation to settle and preventing further abscess formation (Figure 1).
A course of antibiotics may also be required.
Within approximately six weeks, symptoms usually improve significantly, and you will be reviewed by your colorectal surgeon to plan definitive treatment.
At this stage, there are five possible management options:
1. Remove the seton and allow the fistula to heal on its own
2. Leave the seton in place longer or indefinitely, with or without tightening
3. Remove the seton and lay open the fistula tract, dividing muscle
4. Remove the seton and surgically remove the fistula tract, with or without a flap repair
5. Remove the seton and attempt closure using glue or a plug
Excluding Crohn’s Disease
Before proceeding with fistula repair, a colonoscopy is generally recommended to exclude Crohn’s disease. Crohn’s disease is a known cause of anal fistulae, and when present, surgery must be combined with medical treatment to achieve the best outcomes [2].
Treatment Options After Seton Placement
1. Remove the Seton and Allow Spontaneous Healing
If the seton has been in place for up to six weeks and the infection has settled, some surgeons advocate simply removing the seton and allowing the fistula to close naturally. Healing rates of 75–80% have been reported [3,4].
This approach is most successful when the seton is removed before six weeks, as longer periods may allow skin (epithelium) to line the fistula tract, preventing closure.
This option should be used with caution in patients with Crohn’s disease, as recurrence rates are high [5].
2. Leave the Seton in Place (Loose or Tight)
If the fistula involves a significant portion of the anal sphincter muscle, laying it open may risk damage to the muscle and lead to faecal incontinence. In these cases, the seton may be left in place for a longer period or indefinitely.
⦁ Loose seton: Allows ongoing drainage and control of infection
⦁ Tight (cutting) seton: Periodically tightened so it slowly cuts through the muscle over time
With gradual tightening, the seton slowly lays open the fistula tract and eventually falls out without the need for surgical division of the sphincter. This process may take up to a year.
Occasionally, a loose seton may slowly cut through without tightening. Although this may take several years, it is considered safer than a tight cutting seton because it allows the sphincter muscle to heal gradually as the tract opens [6].
3. Remove the Seton and Lay Open the Fistula Tract
If the fistula involves less than one-third of the internal anal sphincter, it may be safe to remove the seton and lay open the fistula tract, dividing the overlying muscle.
This allows the tract to be cleaned (curetted), promoting healing from the inside out. Prior to this procedure, careful assessment using endoanal ultrasound and probing with a Lockhart-Mummery probe is essential to confirm limited sphincter involvement.
4. Remove the Seton and Surgically Remove the Fistula Tract (With or Without a Flap)
If a large portion of the anal sphincter is involved, the seton may be removed and the fistula tract surgically excised. This procedure is best performed after at least 12 weeks, allowing infection to fully settle and the fistula tract to become well defined.
Surgical options include:
⦁ LIFT procedure (ligation and excision of part of the tract without a flap), or
⦁ Complete excision of the fistula tract with flap repair
The type of flap depends on the location of the internal opening:
High internal opening: Rectal advancement flap using rectal mucosa and underlying muscle
Low internal opening: Anoderm V-Y advancement flap
Both approaches involve repair of the sphincter and cleaning (curettage) of the external opening to allow continued drainage while healing occurs.
5. Remove the Seton and Seal the Tract With Glue or a Plug
Various glues and plugs have been developed to seal fistula tracts while preserving the anal sphincter.
Fibrin Glue
Early studies reported healing rates of up to 70%, with no effect on continence. However, longer-term studies have shown high recurrence rates of up to 75% [7].
Fistula Plug
The fistula plug is made of collagen. Initial results were promising [8], but longer-term studies have reported failure rates of 70–80% [9,10].
As a result, plugs are recommended only for selected cases. There is some evidence that longer fistula tracts (>4 cm) are more likely to heal with these techniques [11].
What to Expect Before and After Surgery
Fasting and Bowel Preparation
If you are not having a colonoscopy:
⦁ No bowel preparation is required
⦁ Eat a normal diet the day before surgery
Fasting:
⦁ From midnight if surgery is in the morning
⦁ From 7 am if surgery is in the afternoon
You will be admitted as a day-stay patient and given a Fleet® enema approximately one hour before surgery.
Recovery and Transport
After surgery, you will recover for about one hour until the effects of sedation have worn off. You must not drive yourself home and should arrange for a friend or family member to accompany you.
Bleeding
Minor bleeding or spotting is common for up to five days. This usually occurs after bowel movements. A sanitary pad may be required once or twice daily.
If bleeding exceeds a couple of teaspoons per day, contact your surgeon.
Laxatives
To prevent constipation, regular fibre and stool softenders are recommended for at least one week:
⦁ Psyllium husk (Metamucil® or Fibogel®): 1 tablespoon twice daily
⦁ Stool softener (Coloxyl with Senna®): once or twice daily
Pain Control
Pain is usually managed with:
⦁ Ibuprofen (Brufen®) 400 mg
⦁ Paracetamol, 2 tablets
These should be taken regularly three times daily for five days. Opioid pain relief (Endone) may be prescribed if needed but should be used sparingly, as it can cause constipation.
Antibiotics
You may require antibiotics after discharge to treat ongoing infection. If you have no allergies, this may include:
⦁ Cephazolin (Keflex®)
⦁ Metronidazole (Flagyl®)
Typically prescribed for five days.
Dressings and Seton Care
Some patients require daily wound dressings for up to one week, usually performed by a community nurse or GP.
A thin silastic seton may remain in place to allow ongoing drainage. It is typically reviewed, tightened, or removed at six weeks.
Sitz Baths
Warm to hot salt-water baths are soothing and help keep the area clean.
⦁ Twice daily for one week
⦁ Sit for 10–15 minutes in a shallow bath with a handful of salt
Follow-Up
You will be reviewed by your colorectal surgeon approximately six weeks after surgery to assess healing and discuss any further treatment if required.
References
1. Williams JG, Farrands PA, Williams AB, Taylor BA, Lunniss PJ, Sagar PM, Varma JS, George BD. The Treatment of Anal Fistula: ACPGBI Position Statement. Colorectal Disease. 9 (Suppl. 4): 18-50, 2007.
2. Sands B, Anderson F, Bernstein C, Chey W, Feagan B, Fedorak R, Kamm M, Korzenik J, Lashner B, Onken J, Rachmilewitz D, Rutgeerts P, Wild G, Wolf D, Marsters P, Travers S, Blank M, van Deventer S. Infliximab maintenance therapy for fistulizing Crohn’s disease. The New England Journal of Medicine New England Journal of Medicine. 350 (9): 876–85, 2004.
3. Joy HA, Williams JG. The outcome of surgery for complex anal fistulas. Colorectal Disease. 4: 254-61, 2002.
4. Eitan A, Koliada M, Bickel A, et al. The use of the loose seton technique as a definitive treatment for recurrent and persistent high trans-sphincteric anal fistulas: a long-term outcome. Journal of Gastrointestinal Surgery 2009; 13(6):1116-9.
5. Faucheron JL, Saint-Marc O, Guibert L, et al. Long-term seton drainage for high anal fistulas in Crohn’s disease–a sphincter-saving operation? Diseases of the Colon & Rectum 1996; 39(2):208-11.
6. Lentner A. Wienert V. Long-term, indwelling setons for low transsphincteric and intersphincteric anal fistulas. Experience with 108 cases. Diseases of the Colon & Rectum. 39(10):1097-101, 1996 Oct.
7. Buchanan G, Bartram C, Phillips R, etal. The efficacy of fibrin sealant in the management of complex anal fistula: a prospective trial. Diseases of the Colon and Rectum. 46: 1167-74, 2003.
8. Johnson E, Gaw J, Armstrong D. Efficacy of anal fistula plug vs. fibrin glue in closure of anorectal fistulas. Diseases of the Colon and Rectum 49(3): 371-6, 2006.
9. van Koperen PJ. Bemelman WA. Gerhards MF. Janssen LW. van Tets WF. van Dalsen AD. Slors JF. The anal fistula plug treatment compared with the mucosal advancement flap for cryptoglandular high transsphincteric perianal fistula: a double-blinded multicenter randomized trial. Diseases of the Colon & Rectum. 54(4):387-93, 2011 Apr.
10. Ortiz H, Marzo J, Ciga MA, Oteiza F, Armendariz P, de Miguel M. Randomized clinical trial of anal fistula plug versus endorectal advancement flap for the treatment of high cryptoglandular fistula in ano. Br J Surg. 2009;96:608–612.
11. McGee MF. Champagne BJ. Stulberg JJ. Reynolds H. Marderstein E. Delaney CP. Tract length predicts successful closure with anal fistula plug in cryptoglandular fistulas. Diseases of the Colon & Rectum. 53(8):1116-20, 2010 Aug.