
.
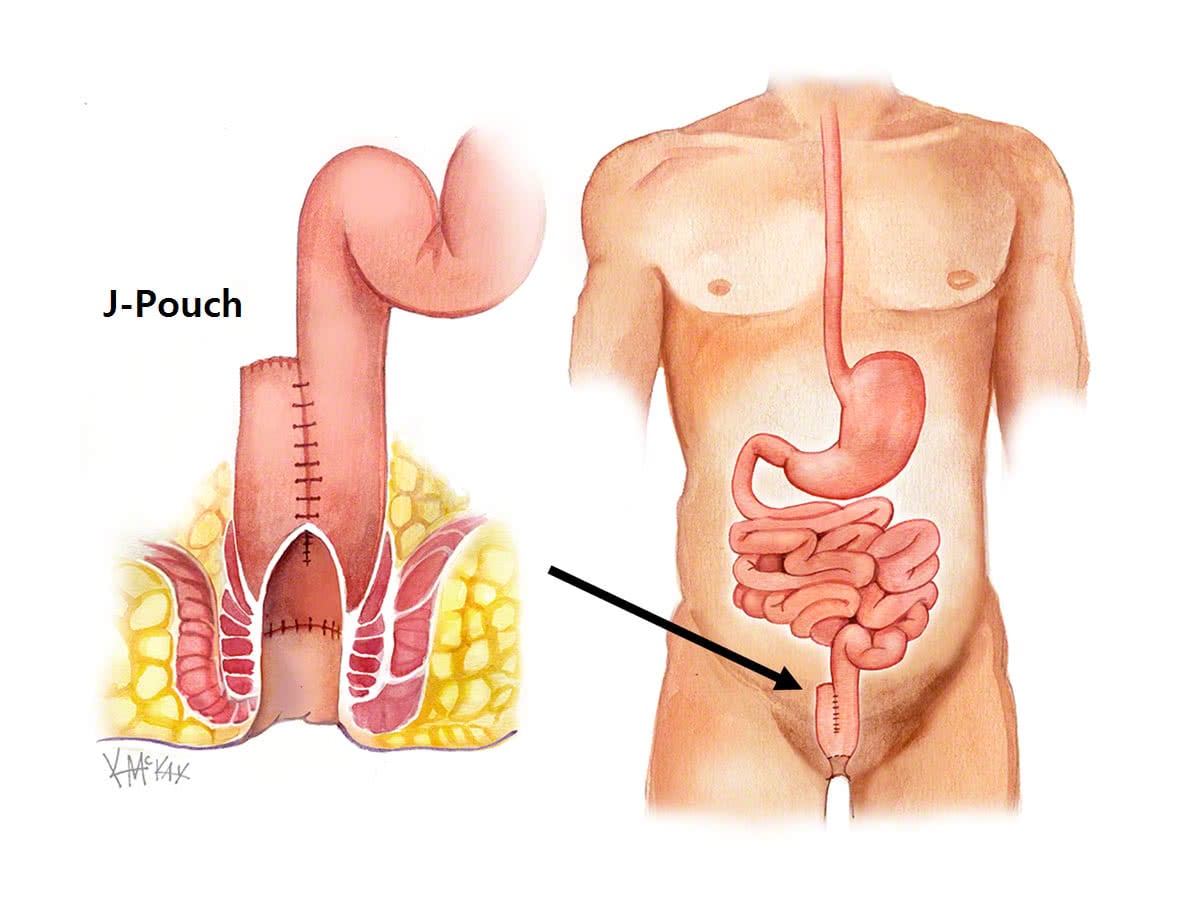
Patients with ulcerative colitis, who have had there colon and rectum removed, may have had their rectum replaced with a “pouch” made of small intestine. When this pouch becomes infected or inflamed, it is referred to as “pouchitis”
Incidence
Pouchitis refers to inflammation of the pouch, with acute pouchitis occurring in 15% of patients with ulcerative colitis.
Management of pouchitis
This usually responds to a course of antibiotics. Antibiotic resistant refractory pouchitis is more difficult to manage, and fortunately less common occurring in only 5% of cases. Other causes for pouchitis may include smoking, poorly controlled disease, or unrecognised Crohn’s disease.
Medical management of pouchitis
Pouchitis usually responds to oral antibiotics (ciprofloxicin or flagyl). Resistant cases require a visit to your colorectal surgeon where a biopsy will be needed. Bacterial overgrowth often responds to Probiotics such as VSL#3®, with the usual dose 6g/day. This contains the health bacteria that normally line the gut and protects against overgrowth by unhealthy bacteria [2-4].
Resistant cases of chronic pouchitis will require the involvement of you gastroenterologist, with consideration of immune modulating agents including steroids such as prednisone, azathoprine, and occasionally infliximab®
Surgery for pouchitis
Occasionally further surgery is required for medically resistant chronic pouchitis. Usually revision surgery is possible, although re-do pouch surgery is sometimes required. On rare occasions, removal of the pouch with formation of a permanent ileosotmy is required.
Reference
- Ahmed AU, Keus F, Heikens JT, et al. Open versus laparoscopic (assisted) ileo pouch anal anastomosis for ulcerative colitis and familial adenomatous polyposis. Cochrane Database Syst Rev. 2009:CD006267.